- Login
- Sign Up
- Online referral form
This site is optimised for modern web browsers, and does not fully support your version of Internet Explorer, some sections of the website may not work correctly such as web forms


CT Guidelines
The accuracy of 3D-printed bones and guides is dependent on a number of factors, including the quality of the original CT data, the parameters used to segment the bone (or other) structures of interest, and the ability of the 3D printer to accurately reproduce the CAD model. Due to the high attenuation coefficient of cortical bone relative to the surrounding soft tissues, bone segmentation is usually an accurate process, as is the final 3D-printing stage (with resolutions of up to 25µm possible with the UV-laser stereolithographic system used to print bones and guides).
These resolutions are significantly in excess of what clinically used CT machines can achieve (usually a minimum slice thickness is 625µm). It follows that acquisition of optimal CT data is the key determinant of the ultimate accuracy of 3D printed bones and guides. When optimised, 3D prints of very small structures are accurate and clinically reliable; for example vertebral drill guides have been used to place 1.5mm pedicle screws as part C1-C2 stabilisation for treatment of atlantoaxial subluxation in Chihuahuas. Conversely, poor CT data can compromise the accuracy of surgical guides would be unreliable.
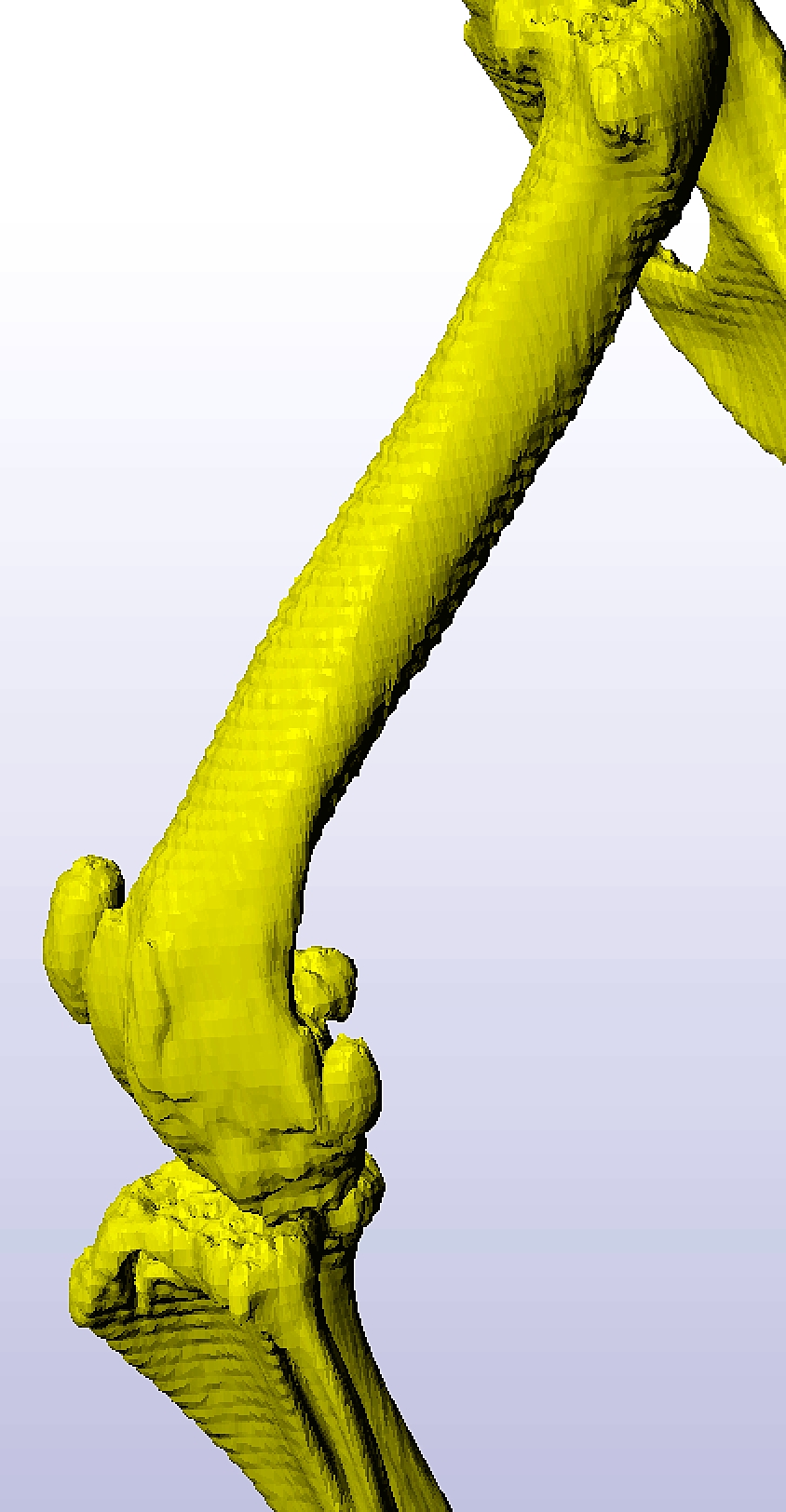
Figure 1 shows stair-step artefact affecting a femur scanned at 45° to the CT gantry with 2.5mm thick slices. In this case the artefact was sufficiently mild than femoral osteotomy guides could be made, however when more severe the true position of the cortices cannot be known even though the irregular appearance can be smoothed in CAD software.
{kind=link}
General CT guidelines -
- Slice thickness -
- In most cases the minimum available slice thickness should be used.
- Occasionally this may adversely affect signal : noise ratio when thicker slices should be used (e.g. big dog cervical and LS spines).
- Field-of-view -
- This should be as small as possible whilst including the area of interest.
- If a large area is necessary (e.g. to assess whole limb conformation) a second scan of a smaller area considered likely to be key may be worthwhile.
- Orientation -
- The key bone(s) of interest should be as perpendicular as possible to the CT gantry.
- Upload the entire bone algorithm DICOM series. It is not necessary to upload soft tissue algorithms.
Area-specific CT guidelines -
Antebrachial deformities
- Include the entire limb with the exception of the scapula, i.e. digits to shoulder.
- The forelimb should be tractioned gently forwards with the patient in sternal recumbency.
- The elbow and carpus should be at the approximate standing angles.
- If the contralateral forelimb has normal conformation which should be scanned separately and submitted.
- It is very helpful to clinically assess the amount of carpal laxity present whilst the dog is sedated.
Other deformities (malunions, other unilateral)
- The affected and contralateral limb should be scanned separately.
- Include the entirety of both limbs.
- The limbs to be scanned should be tractioned gently forwards (forelimbs) or backwards (hindlimbs) with the patient in either sternal or dorsal recumbency.
- For antebrachial and crural deformities it is very helpful to clinically assess the amount of carpal or tarsal laxity present whilst the dog is sedated.
Humeral condyle
- Ideally both elbows should be scanned.
- Include the elbows and the distal half of the humerus.
- The forelimb should be tractioned gently forwards, usually with the patient in sternal recumbency.
- The humerus should be as perpendicular to the gantry as possible (a slight angle is OK).
Medial patellar luxation / DFO
- Ideally scan both hindlimbs separately.
- Optimally include the entire limb (pelvis to digits) to permit assessment of both femoral and tibial deformities.
- The hindlimbs should be tractioned gently backwards with the patient in either sternal or dorsal recumbency.
- Orientate the femur as perpendicular to the gantry as possible.
Vertebrae
- At least a full vertebra on either side of those to be stabilised should be included.
Fractures
- The entirety of the fractured and contralateral bone must be scanned.
- The limbs to be scanned should be tractioned gently forwards (forelimbs) or backwards (hindlimbs) with the patient in either sternal or dorsal recumbency.
Download as PDF
![]()
CT Guidelines
©Copyright 2017 - Vet 3D | Terms & Conditions | Cookie Policy